
By Stephen Spiegelberg, PhD View PDF
Summary
Medical devices, particularly polymeric devices, are frequently augmented (made “radiopaque”) to ensure that they can be visualized when in use or implanted, usually using x-ray. In these cases, radiopacifier, such as barium sulphate, is added to the polymer to increase contrast under medical x-rays, such as fluoroscopy or CT. There is no specific metric for how much contrast is enough, and the level depends on the end use and indications, but there exists an ASTM standard that quantifies the relative “radiocontrast” of the device. The reported radio contrast is frequently then used in comparison to materials intended to represent the target body area. This application note describes the method of measuring the radiopacity of materials using ASTM F640.
Background

Figure 1: X-ray image of external electrodes on patient.
For positioning and tracking of permanent and temporary medical devices such as hip and knee replacements, catheters, stents, dental components, and screws, the device is often implanted or constructed with a radiopacifier or marker. X-ray and fluoroscopy are commonly used to visualize the device. To visualize the component, the electron density of the component must be different from the surrounding tissue, be it soft tissue (skin, muscle, organs), or hard tissue (bone). An example of the value of this approach to the surgeon is shown in Figure 1 where the electrodes would be invisible on the x-ray without a contrast agent and the bones image differently than the tissue and electrodes.
Medical devices often incorporate a material or construct that will partially or totally block the transmission of electromagnetic radiation in the form of X-rays through the device. These materials are often termed radiopacifiers and are “radiopaque”, as opposed to radiolucent materials that freely allow the passage of X-rays. On an analog X-ray film, a radiopaque material will appear white because it has blocked any exposure of the film, while on a digital X-ray, it will generally appear dark gray or black, because it represents an area of no exposure. The two styles of X-ray image are therefore usually the reverse of each other, although the digital image can readily be inverted to match the film.
Most metals possess a high electron density and are therefore naturally radiopaque relative to tissue. Often, strands or beads made of tantalum are incorporated into devices to permit the radiologist, surgeon, or X-ray technician to visualize the position of the device, as well as track its movement. For materials that are not intrinsically sufficiently radiopaque, such as polymers, elastomers and cements, minerals such as barium sulfate, zirconium oxide, and bismuth are often incorporated.
When designing new devices, quantitative measurements of the radiopacity of the material can aid in design characteristics and regulatory approval, as well as product differentiation. ASTM F640 “Standard Test Methods for Determining Radiopacity for Medical Use” is a commonly used technique for quantifying the radiopacity of medical devices, as well as non-medical devices.
Procedure
In ASTM F640, a device is imaged in an X-ray system. Included in the image is an aluminum step wedge of known, precisely machined thickness from a specific alloy (see Figure 2), as it is known that different alloys have differing radiopacities.[1] The X-ray image is collected at clinically relevant doses. A layer of material can be laid over the samples to simulate the tissue layer that would be over the device when in use, such as vascularity, skin, and muscle tissue for a catheter used in the arm or leg, or bone tissue for devices used in the chest or pelvis. This layer is called a ‘body mimic’ and can either be a material designed to have a similar radiopacity to the tissue in question, or it could be cadaveric or animal tissue. This step is important because the apparent radiopacity is not simply cumulative because as the beam interacts with the device and mimic the photons lose energy and their penetration depth changes. Often, researchers will use 5 or 10 mm aluminum plate as a body mimic.
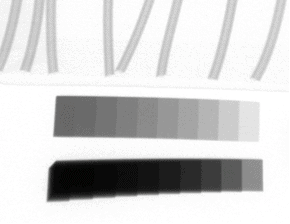
Figure 2: X-ray image shown two step wedges (bottom) of different thickness ranges, and tubing samples for analysis (top).
After the X-ray is obtained, the pixel intensity of the step wedge as a function of each step thickness, relative to the background, is determined, as shown in Figure 3. The thicker the step, the darker the image, and the greater the pixel intensity difference from the adjacent background. Figure 3 demonstrates a calibration curve for images collected with and without a body mimic and demonstrates the attenuating effects of the body mimic.
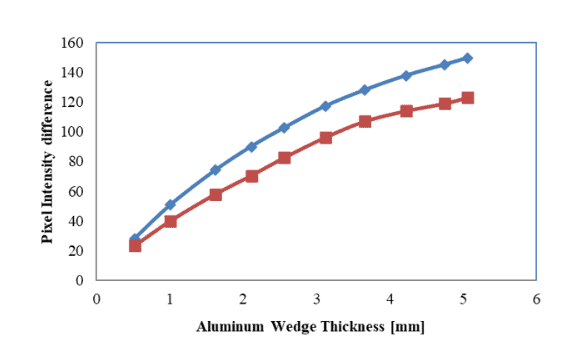
Figure 3: Pixel intensity calculation for aluminum wedge calibration. The blue diamonds are obtained without a body mimic. The red squares represent the same wedge in the presence of a body mimic.
The sample is then analyzed, measuring the relative pixel intensity for each specimen point and then converting this intensity into an equivalent aluminum thickness. In the tubing samples in Figure 2, the equivalent aluminum thickness was 0.95 mm. With this approach, different X-ray systems will produce comparable radiopacity measurements.
Conclusions
The importance of a reliable means of determining how a device responds under x-ray is obvious. Although there are parameters that define exactly how “radiopaque” a material is (known as Hounsfield units), this calculation is complex. ASTM F640 uses a relatively simple means of determining relative contrast and provides a mechanism for rapidly determining relative performance of materials and completed devices. It is therefore an invaluable tool for medical device developers and manufacturers.
Who We Are
CPG is healthcare-focused material science R&D company with extensive experience in developing and testing medical devices. Our broad experience in material science selection and consulting is supported by a broad analytical expertise and capability of which radiopacity is only one. Please contact us for more information on how we can assist your team.
[1] Watts, D.C., McCabe, J.F., Aluminum radiopacity standards for dentistry: an international survey, J. Dent., vol 27(1), 73-78 (1999).